Scene 1 (0s)
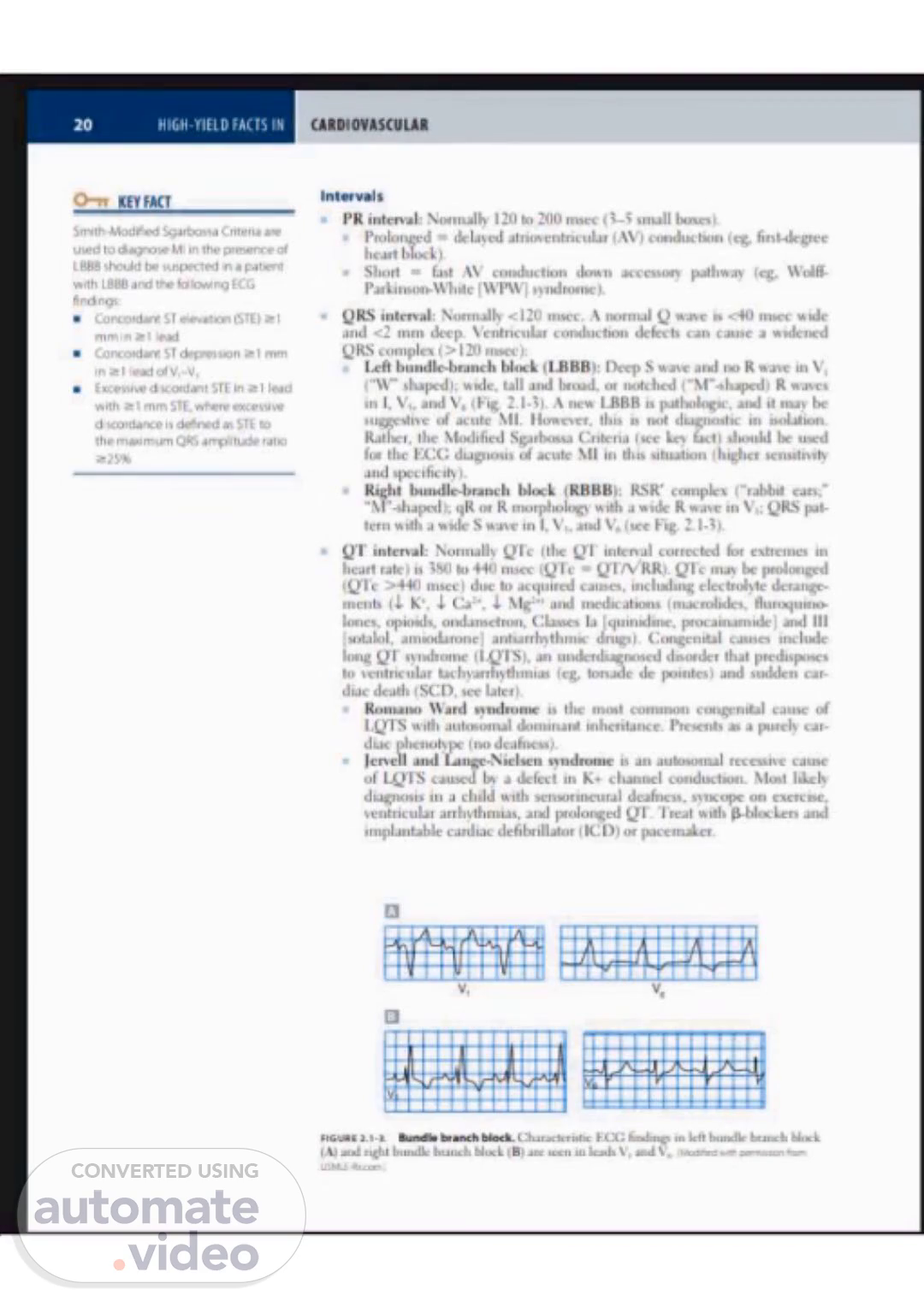
HIGH-YIELD FACTS IN O-n KEY FACT Smith Modified Sgartxh%a Cntena ate used to In the pre•.ence oi LBBB tx• suspected in a patent With LBBB and the ECG • Concordant ST e/evation (Sto Concordant degresson mm • STE in 21 lead With t mm STL where exceisive d wordarve is as to the maximum QRS ampbn*je tato intervals PR interval: Normallv 120 to 200 lunes). • Prolonged delayed atrioventricular (AS') conduction first-degree heart block). • Short • fast AV conduction down accessory pathway Wolff• Parkinson-mute ( WEAVI 'YidtOme). QRS interval: Normallv < 120 msec, A normal Q is 40 rns.c•c wide and tntn deep. Ventneular conductu»n defects can cause a wulcned QRS cotnple\ > 1 20 tnsec i: bundle-branch block (I.BBB): S wave no R wave in V. shaped); wvde. tall broad. ot notched ( -M --•hape•di R in l. and VL 2.13), A I-BBB it mav of acute MI. Ilowe•er. this not diagnostic in isolation. Rather. the Modified Sgatb€nsa C.rttena (see fact' should be for thc ECG dugnosis acute MI in this situation and specificity), Right bundle-branch block (RBBB): RSR• complex ("rabbit " 'M "-shaped); qR ot R morpholog••. With a R wave •n VI; QRS pat- tern with a wide S wave in l, and V'. (see Fig. 2. interval: Normally (the intenul corrected extremes in heart rate j to 440 (Q'l•c •z RR)_ el-c may prolonged msec) due to acquired causes. including electrolyte derange- menb K•. Ca:•, Mg:•• and tncd•cattons (nucrolidcs. lones. ondansetron. Classes procatnarrudcl and Ill Isotalol, atniodaroncl drugs). Ccmgc•nital long syndrome an underdiagnosed doordcr that to vcntnculat (eg. tots.•dc dc Biintes) and suddcti car- doc death (SC.D. see later). Romano Ward syndrome is the most common cause of ILYIS With dotnjnant inheritance. Presents as a purely car- phenoftpe I no deafness). • Jenell and IangeNielsen syndrome is an autosomal recessise cause of Lei S caused by a defect in K• channel conduction. Most diagnosis in child With sensorineural deafness. s'tkopc on exercise. ventricular arrhvthmus. and prolonged Treat With and implantable cardiac defibrillator ICD) or pacemaker. v, 2. Characteristic fndtn. in left.
Scene 2 (2m 32s)
[Audio] The ECG changes observed in cases of acute ischemia include peaked T-waves and ST.
Scene 3 (2m 40s)
[Audio] Slide number 3 out of 5 discusses the use of Smith Modified Sgartxh%a Cntena in diagnosing certain heart conditions involving LBBB and ECG readings. Specifically, the mnemonic "D-ARMS PITS" helps us remember high-yield facts when assessing for murmurs. It is essential to have a thorough understanding of murmurs when diagnosing heart conditions, making the Smith Modified Sgartxh%a Cntena a valuable tool. This mnemonic divides murmurs into two categories: diastolic and systolic. Starting with diastolic murmurs, the "D" in D-ARMS represents the time period in the cardiac cycle when the heart is relaxing and filling with blood. The "ARMS" stands for different types of diastolic murmurs: Aortic regurgitation, Mitral stenosis, Pulmonary regurgitation, and Tricuspid stenosis. Moving on to systolic murmurs, the "S" in D-ARMS represents the time when the heart is contracting and pumping blood out. The "ARMS" helps us remember the different types: Aortic stenosis, Mitral regurgitation (or prolapse), Pulmonary stenosis, and Tricuspid regurgitation. Other key points related to cardiovascular conditions include right ventricular hypertrophy (RVH), often caused by pulmonary hypertension, pulmonary embolism, or heart disease. On an ECG, RVH is indicated by an R wave in V1 greater than 7mm and a dominant R wave in V6. During a physical exam, certain findings can help narrow down potential diagnoses. These include jugular venous distention (JVD), which is an increase in the jugular vein when the head of the bed is elevated, usually indicating volume overload and potentially right heart failure or pulmonary hypertension. Another important finding is hepatojugular reflux, seen when neck veins distend with pressure on the abdomen, often present in the same conditions as JVD. Lastly, Kussmaul's sign is a rise in jugular venous pressure with inspiration, commonly associated with constrictive pericarditis. When it comes to murmurs, a flow murmur is a soft murmur that is position-dependent and generally not indicative of any cardiac disease, while a gallop rhythm is a sign of potential heart disease..
Scene 4 (5m 0s)
[Audio] Please provide the answer and I will wait for your response..
Scene 5 (5m 35s)
[Audio] The presentation discusses the importance of recognizing certain murmurs and physical examination findings in diagnosing and managing various cardiovascular conditions. Key points include: * Recognizing murmurs such as holosystolic murmurs, mid-diastolic murmurs, and systolic murmurs, which can indicate conditions like aortic regurgitation.