Imaging of Urinary System
Scene 1 (0s)
Imaging of Urinary System. Dr. Dilgash Hameed Ahmad M.Sc. Diagnostic Radiology.
Scene 2 (11s)
Outline. Imaging modalities in Radiology Radiological terms Imaging modalities of urinary system Radiological anatomy of urinary system.
Scene 3 (40s)
Learning objectives. Be familiar with the imaging techniques used in evaluating the urinary system. Be familiar with the normal radiological appearances of different urinary tract structures. Be able to identify urinary tract structures on different imaging modalities..
Scene 4 (41s)
Imaging Modalities of Radiology. Conventional radiography (X-ray) Ultrasound Computed Tomography (CT scan) Magnetic Resonance Imaging (MRI) Fluoroscopy Angiography.
Scene 5 (5m 41s)
Radiological Terms. X-ray – density Ultrasound – echogenicity Hypoechoic Hyperechoic Isoechoic Echogenic Anechoic.
Scene 6 (7m 44s)
Main Imaging Modalities of Urinary System. aNnosvunn xvu•x NVOS 10.
Scene 7 (7m 46s)
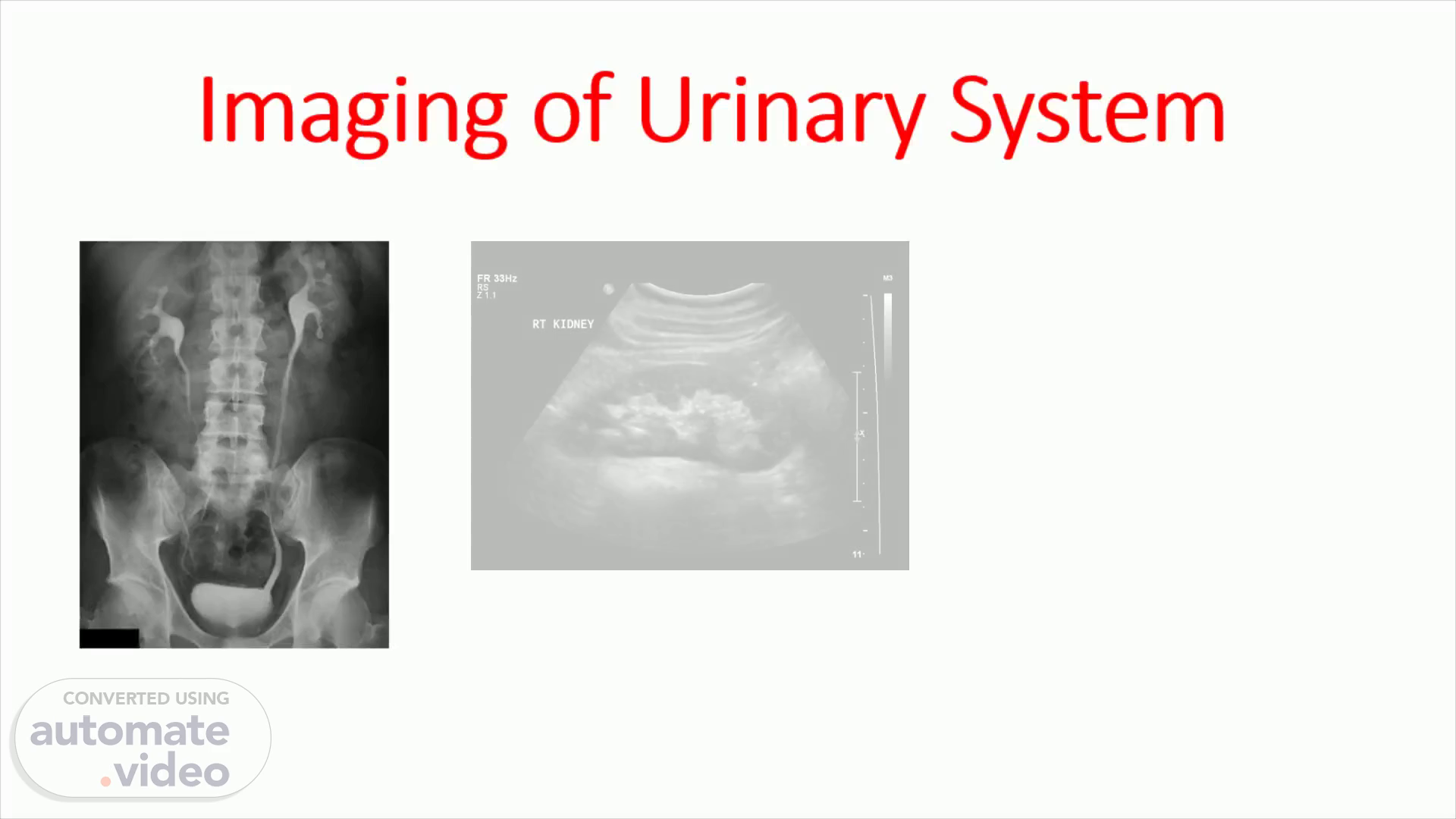
US: Ultrasound First-line investigation in most patients. Safe , no risk of radiation. Uses of US: Assesses the size, shape, location, and blood flow to the kidneys (assesses blood flow to the kidneys using doplar ultrasound using color ultrasound) . Assesses the prostate gland in males. Detects stones, hydronephrosis and hydroureter , cysts, solid masses, infective changes..
Scene 8 (8m 49s)
Calyces Abd — c60 Gerota's fascia 0.8 Cortex 13 Renal Pelvis.
Scene 9 (9m 56s)
KUB: Kidneys, Ureters, Bladder Rapid plain x-ray but has risk of radiation exposure. Uses of KUB: General evaluation mainly for stones; also detects calcifications. May show soft tissue shadows (psoas abscess). Assess bones. Assess site of drains or stents..
Scene 10 (11m 7s)
Liver Right Kidney Hepatic Flexure Psoas Muscle Ascending Colon 5th Lumber Vertebrae Sacrum wiki Spleen Splenic Flexure Left Kidney 12th Rib Psoas Muscle Descending Colon Iliac Wing Left Femur Symphysis Pubis.
Scene 11 (13m 1s)
IVU: Intravenous urography Timed series of x-ray images of the urinary tract after administration of IV contrast agent. Gives detailed information about the pelvicalyceal system (PCS) and ureters . Indications: To assess patients with anatomic variations or congenital anomalies. Acute ureteric colic, stones, and hematuria..
Scene 12 (14m 9s)
Phases of IVU. Nephrogram –1-3 minutes Pyelographic – 10-15 minutes Ureterogram – 30 minutes Cystogram – 45 minutes Post-void.
Scene 13 (14m 25s)
. Nephrogram phase 1-3 mins. rrp-n-n-n-n-rn-n-p-rn-p-rn-p-n-rp-l.
Scene 14 (14m 49s)
__OLuå-J\. . IVU. Ureterogram phase 30 mins. Cystogram phase 45 min.
Scene 15 (19m 22s)
CT scan: Computed Tomography Indications : Evaluation of masses Staging of tumors Diagnosis or exclusion of renal trauma Demonstration of radiolucent stones Delineation ( رسم ) of renal vascular anatomy In some centers, to assess acute ureteric obstruction.
Scene 16 (21m 2s)
Other imaging modalities. Used in selected cases….. MRI & MRA: Magnetic Resonance Imaging & Angiography Clarify problems not solved by US or CT Reserved mainly for vascular problems (renal artery stenosis, venous extension in tumor, vasculature before surgery). Antegrade & Retrograde Pyelography Reserved for cases where less invasive procedures failed to reach diagnosis especially in obstruction. Cystography, Urethrography & Micturating Cystourethrography (MCUG) Used mainly in reflux. Urethral abnormalities (stricture, valve). Functional bladder diseases..
Scene 17 (21m 24s)
Radiological Anatomy of Urinary System.
Scene 18 (21m 30s)
Kidneys. KUB: Soft tissue density with lucent outlines (due to perirenal fat) . Renal size: range from 10-15 cm , left is usually larger. US: Renal outline is normally smooth. Size: smaller than on KUB, 9-12 cm . Renal cortex (parenchyma) appears darker than the renal sinus (fat, calyces, infundibula, and vessels) which is very bright (echogenic)..
Scene 19 (21m 57s)
Kidneys. IVU: Renal outline is seen in nephrogenic phase. Calyceal system is seen in pyelographic phase..
Scene 20 (22m 4s)
Kidneys. CT and MRI: Kidneys are seen as slices from T12-L3 vertebral levels. They are homogeneous on unenhanced CT images. On MRI , the cortex and medulla appear different on T1 and T2 weighted images… T1: cortex is higher in signal (hyperintensity mean whiter) than medulla. T2: cortex is lower (hypointensi mean less whiter) in signal than medulla.
Scene 21 (23m 20s)
Kidneys. On both CT and MRI three phases of contrast enhancement can be appreciated: Arterial cortico -medullary phase – cortex enhances strongly so cortico -medullary junction is well differentiated. (we take picture after 20-30 sec of injecting the contrast) Venous nephrogenic phase – homogeneous contrast throughout the kidney. (we take picture after 60-100 sec of injecting the contrast) Delayed excretory phase – contrast is seen in collecting system. (we take picture after 6-10 minute of injecting the contrast).
Scene 22 (26m 0s)
Ureters. KUB: Ureters are not visualized on plain films. Course: they pass anterior to tips of the transverse processes of L2-L5 vertebrae at ischial spines and medially again to the bladder. US: The proximal and distal parts may be visible when dilated. Mid-portion is not usually seen due to gaseous reflections unless abnormally dilated..
Scene 23 (26m 23s)
Ureters. IVU: Are usually partially visualized when filled with contrast due to peristalsis. Course: same as on KUB . CT scan: Ureters can be identified even on non-contrast images. Normal diameter: up to 3 mm but normally has three regions of constrictions..
Scene 24 (26m 29s)
Urinary Bladder. Plain films: Smooth and rounded soft-tissue density with surrounding lucent line. Contrast studies: Fills with contrast either after IV injection in IVU or retrogradely via the urethra. Uterine and prostatic impressions are seen at postero -superiorly and inferiorly , respectively..
Scene 25 (27m 43s)
Urinary Bladder. Ultrasound: Anechoic fluid filled structure. Normal wall thickness: 3-5 mm. CT scan: Fluid density on non-contrast images. Hyperdense on contrast enhanced images. MRI: T1: bladder wall and contents are homogeneous low signal. T2: wall is low signal and urine is high signal..
Scene 26 (29m 23s)
Male Urethra. Retrograde urethrography : Urethra is outline by contrast, verumontanum appears as a posterior filling defect in prostatic urethra..
Scene 27 (30m 37s)
Prostate Gland. Ultrasound: Peripheral zone – isoechoic Central part – hypoechoic CT scan: Rounded soft-tissue density. Zonal anatomy cannot be distinguished..
Scene 28 (31m 22s)
Prostate Gland. MRI: T1: low signal intensity, zones cannot be distinguished. T2: is excellent for zonal anatomy. Peripheral zone – high signal. Transitional & central zones – intermediate signal..
Scene 29 (31m 48s)
Gallery.
Scene 30 (31m 55s)
CT vs MRI.
Scene 31 (33m 51s)
TRANS BLADDER. AD omen • Har•low Pwr Gn 3 cg M' SRI 11 1 J CRI t.
Scene 32 (35m 27s)
SMV. Colon Liver Liver is ancreas Duodenum Adrenal Spleen Vena Cava nf.andanteriort g I Right Kidney 1 r ug in supine position. ver with patient.
Scene 33 (37m 2s)
Fornix Minor calyx Major calyx pelvis Ureter. Renal Calyx A'.-Renai Pelvis ——psoas Bladder.
Scene 34 (37m 44s)
Fat Perinephric fat appears white in MR. Kidneys are surrounded by perinephric fat. Fat appears dark in CT. ONE BREATH HOLD RENAL 3MNlPAQlJE Fat VV398.
Scene 35 (38m 1s)
Ureters carry urine from renal pelvis to the bladder 25 to 30 cms long. They pass in front of psoas muscle and in close proximity to transverse process of vertebrae In trauma if there iSany fractureoftransverse process we need to evaluate for injury to ureters. Uretersare small and may not be yjsualized in,its entirety because of peristaltic-activi . IVPAÅ CT arecjdeälto visyalize dilate&urete US snofgo for urete unless Cheyaeeryfdil ted. Dilated Ureter Normal Ur ter Psoas.
Scene 36 (39m 33s)
urn Is sterior to bladder. Uterus is superi r b d$ bladder is emptied prio{ to tranS v inai of the uterus and ovaries. Bladd 'å nsabddminql approac of the is filled varie Prostate inferio bla d uterus a in males Uterus Bladder Rectum.
Scene 39 (42m 28s)
eseq lepeuv. CT without contrast.
Scene 40 (42m 41s)
Portal venous phase.
Scene 41 (43m 0s)
•v 00 d.